
این مقاله به بررسی سندرم ایزوله رادیولوژیک (RIS) در کودکان میپردازد. RIS به شرایطی گفته میشود که در آن، بدون وجود هرگونه علائم بالینی مربوط به بیماریهای دمیلینهکننده سیستم عصبی مرکزی (مانند اماس)، تصاویر MRI مغز یا نخاع، نشانههایی مطابق با این بیماریها را نشان میدهند.
مطالعه و روشها
این تحقیق یک مطالعه کوهورت چندمرکزی بر روی ۳۸ کودک (۲۷ دختر و ۱۱ پسر) از ۶ کشور بود که بهطور تصادفی و معمولاً به دلایلی مانند سردرد (۵۳٪ موارد)، مورد اسکن MRI قرار گرفته و یافتههای تصویربرداری آنها ویژگی (DIS) در اماس را داشت. این کودکان بهطور متوسط به مدت ۴.۸ سال پیگیری شدند.
یافتههای کلیدی
- ۴۲٪ از کودکان (۱۶ نفر از ۳۸ نفر) در مدت میانه ۲ سال پس از اولین MRI، یک حمله از جمله نوریت اپتیک، میلیت یا درگیری ساقه مغز را تجربه کردند.
- ۶۱٪ از کودکان (۲۳ نفر از ۳۸ نفر) در مدت میانه ۱.۱ سال، شاهد پیشرفت ضایعات در تصاویر MRI بعدی بودند (ظهور ضایعات جدید T2 یا ضایعات enhance شونده).
- عوامل خطر پیشبینیکننده: دو عامل بهطور مستقل با افزایش خطر بروز حمله بالینی اولیه مرتبط بودند:
- وجود دو نوار اولیگوكلونال یا بیشتر در مایع مغزی-نخاعی (CSF) (با نسبت خطر ۱۰.۹)
- وجود ضایعات در نخاع در MRI (با نسبت خطر ۷.۸)
نتیجهگیری
این مطالعه نشان میدهد که RIS در کودکان یک وضعیت پرخطر است و سیر بالینی و رادیولوژیک سریعتری نسبت به بزرگسالان دارد. بخش قابلتوجهی از این کودکان در طول زمان به علامت دار میشوند یا ضایعات مغزی/نخاعی آنها پیشرفت میکند. وجود نوارهای اولیگوکلونال در مایع مغزی-نخاعی و ضایعات نخاعی، شاخصهای مهمی برای شناسایی کودکان در معرض خطر بالاتر هستند. این یافتهها بر لزوم پیگیری منظم و دقیق کودکان مبتلا به RIS و همچنین انجام مطالعات بیشتر برای تأیید این نتایج و تدوین راهنمای بالینی برای مدیریت این بیماران تأکید میکند.
ABSTRACT
Objective: To describe clinical and radiologic outcomes of children with incidental findings on neuroimaging suggestive of CNS demyelination (termed “radiologically isolated syndrome” or RIS).
Methods: Clinical and radiologic data were obtained from a historical cohort of children with no symptoms of demyelinating disease who had MRI scans that met the 2010 MRI criteria for dissemination in space for MS.
Results: We identified 38 children (27 girls and 11 boys) with RIS now being prospectively followed at 16 sites in 6 countries. The mean follow-up time was 4.8 ± 5.3 years. The most common reason for initial neuroimaging was headache (20/38, 53%). A first clinical event consistent with CNS demyelination occurred in 16/38 children (42%; 95% confidence interval [CI]: 27%-60%) in a median of 2.0 years (interquartile range [IQR] 1.0-4.3 years). Radiologic evolution developed in 23/38 children (61%; 95% CI: 44%-76%) in a median of 1.1 years (IQR 0.5-1.9 years). The presence of ≥2 unique oligoclonal bands in CSF (hazard ratio [HR] 10.9, 95% CI: 1.4-86.2, p = 0.02) and spinal cord lesions on MRI (HR 7.8, 95% CI: 1.4-43.6, p = 0.02) were associated with an increased risk of a first clinical event after adjustment for age and sex.
Conclusions: We describe the clinical characteristics and outcomes of children with incidental MRI findings highly suggestive of CNS demyelination. Children with RIS had a substantial risk of subsequent clinical symptoms and/or radiologic evolution. The presence of oligoclonal bands in CSF and spinal cord lesions on MRI were associated with an increased risk of a first clinical event. Neurol Neuroimmunol Neuroinflamm 2017;4:e395; doi: 10.1212/NXI.0000000000000395
GLOSSARY
CI = confidence interval; DIS = dissemination in space; HR = hazard ratio; IQR = interquartile range; RIS = radiologically isolated syndrome.
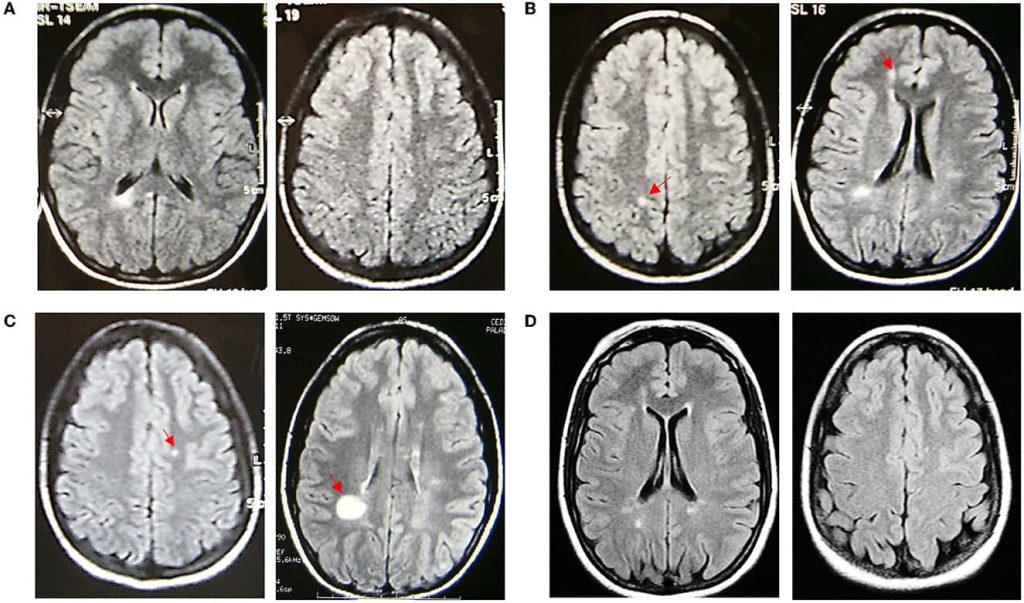
The incidental finding of abnormalities on MRI scans of the brain and spinal cord has become more common due to the increasing use of MRI in the evaluation of a wide range of medical conditions in children.¹² Some of these abnormalities are highly suggestive of CNS demyelination based on their size, location within the white matter, and shape. This finding has previously been described in adults and has been termed “radiologically isolated syndrome” or RIS.³⁻⁵ Criteria for RIS in adults were proposed in 2009 and require both clinical and imaging factors including the incidental detection of MRI abnormalities meeting the following criteria: (1) ovoid and well-circumscribed homogenous foci with or without involvement of the corpus callosum, (2) T2 hyperintensities ≥3 mm in diameter fulfilling at least 3 of the 4 Barkhof MRI criteria for dissemination in space (DIS), as adopted in the 2005 diagnostic criteria for MS,⁶ and (3) the CNS abnormalities are not consistent with a vascular pattern.³ We recently reported a teenager with such incidental white matter abnormalities detected on brain MRI.⁷ However,
Author affiliations are provided at the end of the article.
Co investigators are listed at Neurology.org/m.
Funding information and disclosures are provided at the end of the article. Go to Neurology.org/m for full disclosure forms. The Article Processing Charge was funded by the authors.
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License 4.0 (CC BY-NC-ND), which permits downloading and sharing the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal.
You can read the full text of the article in the pdf file.